Statin Interactions and Myopathy Risk: What You Need to Know

Statin Myopathy Risk Calculator
Statins save lives. Millions of people take them every day to lower cholesterol and prevent heart attacks and strokes. But for some, the cost is muscle pain - sometimes severe enough to stop the medication entirely. The real danger isn’t just the statin itself. It’s what happens when it mixes with other drugs. That’s where the risk of myopathy spikes - a condition that can turn from mild soreness to life-threatening muscle breakdown in a matter of days.
What Exactly Is Statin-Induced Myopathy?
Myopathy means muscle disease. In the case of statins, it’s when muscle fibers start breaking down. You might feel soreness, weakness, or cramps - especially in your thighs, shoulders, or lower back. These symptoms don’t always show up right away. Sometimes they creep in after weeks or months. The real red flag? A blood test showing creatine kinase (CK) levels more than 10 times the normal upper limit. That’s when it crosses into clinical myopathy. Worse still, if muscle cells spill their contents into the bloodstream, you risk rhabdomyolysis - a rare but deadly condition that can wreck your kidneys.Here’s the catch: most people who take statins never get this. Studies show the risk of serious muscle damage is less than 0.1% per year. But for certain people - especially those on the wrong statin, the wrong dose, or mixing it with other meds - that risk can jump 10-fold.
Not All Statins Are Created Equal
There are six main statins on the market. They might all lower cholesterol, but they don’t all carry the same muscle risk. The difference comes down to how they’re processed by your liver and how easily they enter muscle tissue.- Lipophilic statins - like simvastatin, lovastatin, and atorvastatin - slip easily into muscle cells. That’s why they’re linked to higher rates of muscle pain.
- Hydrophilic statins - like pravastatin, rosuvastatin, and fluvastatin - stay mostly in the liver. They’re less likely to cause muscle issues.
Real-world data tells the story. Pravastatin has a myalgia rate as low as 0.6% to 1.4%. Rosuvastatin? Up to 12.7%. Simvastatin at 80mg carries a 0.44% annual risk of myopathy. That’s 20 times higher than low-dose pravastatin. And don’t be fooled by brand names - generic simvastatin is just as risky.
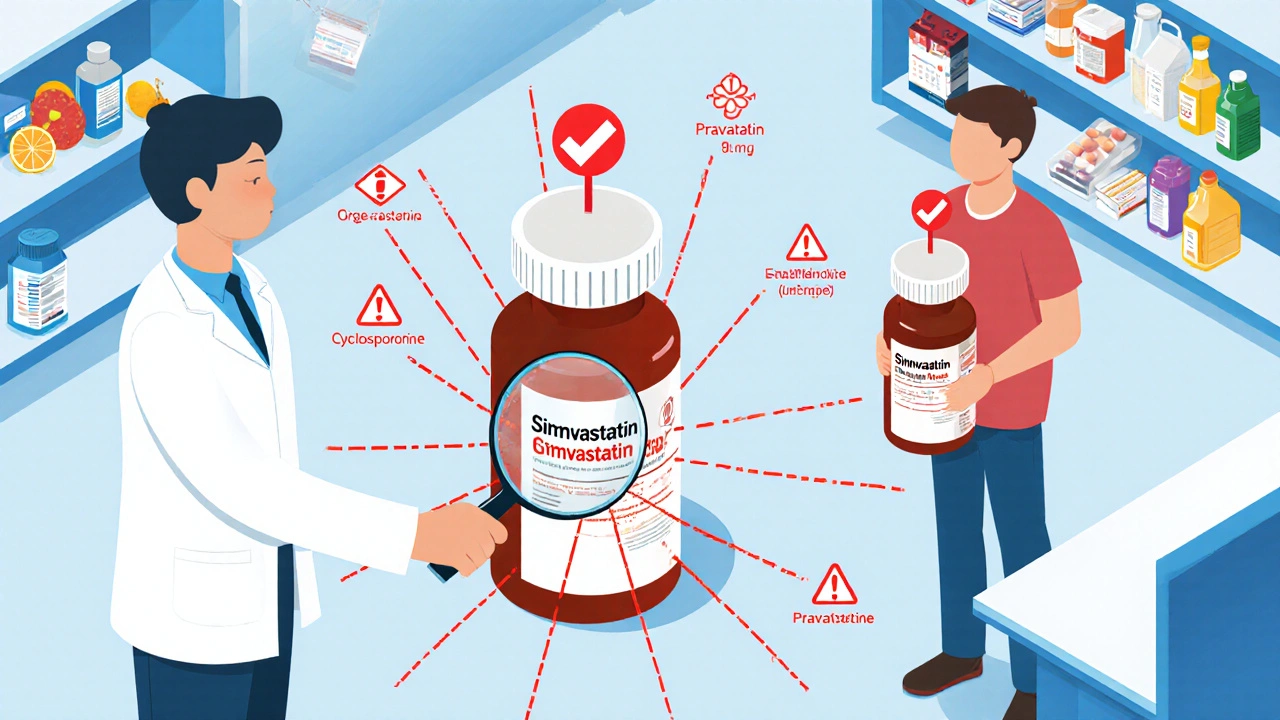
Drug Interactions That Raise the Risk
The biggest danger isn’t statins alone. It’s what you take with them. Certain drugs block the liver enzymes that break down statins. That causes statin levels to build up in your blood - like turning up the volume on a song until it distorts.Here are the top offenders:
- Macrolide antibiotics - clarithromycin and erythromycin. These are common for sinus infections and bronchitis. They can make simvastatin levels spike by 10 times. Atorvastatin? Up to 4 times. Azithromycin? Safe. No interaction.
- Fibrates - gemfibrozil is the worst. It doubles statin levels. Fenofibrate? Much safer. If you need both, go with fenofibrate.
- Cyclosporine - used after organ transplants. Can boost statin levels by 3 to 13 times. This combo is a minefield.
- Calcium channel blockers - diltiazem and verapamil. These are common for high blood pressure. The FDA now limits simvastatin to 20mg if you’re on either.
- Amiodarone - for irregular heartbeat. Also forces a statin dose cut.
And here’s what you should know: if you’re on one of these drugs, you don’t need to stop your statin forever. You just need to switch to the right one. Pravastatin, rosuvastatin (at 20mg or less), or fluvastatin are safer choices. Your doctor can keep you on cholesterol control without risking your muscles.
Who’s Most at Risk?
Some people are just more vulnerable. Age, body size, and health conditions stack the deck:- Over 75 years old
- Small frame or low body weight
- Chronic kidney disease
- Hypothyroidism (underactive thyroid)
- Heavy alcohol use
- Intense exercise - especially if you’re not used to it
- Genetics - a variant in the SLCO1B1 gene makes simvastatin 4.5 times more likely to cause muscle damage
It’s not just one thing. It’s the combo. An 80-year-old woman with kidney issues taking simvastatin and diltiazem? That’s a perfect storm. She might never have had muscle pain on statins alone - but together, the risk becomes real.
What to Do If You Have Muscle Pain
If you start feeling unusual muscle soreness - not from a workout, not from an injury - don’t ignore it. Talk to your doctor. Get a blood test for creatine kinase. If it’s over 10 times the upper limit, your statin should be stopped. If it’s between 5 and 10 times, your doctor might pause it temporarily and retest.Here’s what works in practice:
- Stop the statin for 2-4 weeks. See if symptoms improve.
- If they do, restart a different statin - preferably pravastatin or low-dose rosuvastatin.
- If symptoms return, you’ve likely got statin-associated muscle symptoms (SAMS). That’s a real diagnosis, not just “side effects.”
Studies show 71% of people who thought they were “statin intolerant” could tolerate a different statin at a lower dose. Don’t give up on cholesterol control just because one statin didn’t work.

Alternatives When Statins Aren’t an Option
If you’ve tried multiple statins and still get muscle pain, you’re not out of options. Bempedoic acid (brand name Nexletol) is a newer drug that lowers cholesterol without entering muscle tissue. It’s not a statin, so it doesn’t cause myopathy. But it costs over $4,000 a year - versus $6.60 for generic atorvastatin. Insurance often won’t cover it unless you’ve failed statins.Other options include ezetimibe, PCSK9 inhibitors (injections like Repatha or Praluent), or icosapent ethyl (Vascepa). These aren’t first-line, but they’re proven for people who truly can’t tolerate statins.
How to Stay Safe
You don’t need to fear statins. You need to be smart about them. Here’s your action plan:- Always tell your doctor and pharmacist about every medication you take - including over-the-counter drugs, supplements, and herbal remedies.
- If you’re prescribed an antibiotic like clarithromycin or erythromycin, ask: “Is this safe with my statin?” If you’re on simvastatin or lovastatin, pause it during the course.
- Ask for pravastatin or low-dose rosuvastatin if you’re on a high-risk drug like diltiazem or cyclosporine.
- Get a baseline CK test before starting a statin - especially if you’re over 70 or have kidney issues.
- Don’t take coenzyme Q10 hoping it’ll fix muscle pain. The evidence is weak. But if it helps you sleep better? No harm.
Statins are still the most effective tool we have to prevent heart disease. The benefits far outweigh the risks - for most people. But those risks aren’t random. They’re predictable. And with the right knowledge, they’re avoidable.
Can I take statins with grapefruit juice?
Grapefruit juice can interfere with how your body breaks down certain statins, especially simvastatin, lovastatin, and atorvastatin. It blocks an enzyme in your gut that normally breaks down these drugs, leading to higher blood levels. A single glass can increase statin exposure by up to 15 times. Avoid grapefruit juice entirely if you’re on one of these statins. Pravastatin, rosuvastatin, and fluvastatin are safe.
Does taking statins at night reduce muscle pain?
No. The idea that taking statins at night reduces muscle pain comes from older statins like lovastatin and simvastatin, which work best when taken at night because your liver makes more cholesterol then. But muscle pain isn’t tied to timing - it’s tied to the drug’s chemical properties and interactions. Taking your statin in the morning or evening won’t prevent myopathy.
Are natural supplements like red yeast rice safer than statins?
Red yeast rice contains monacolin K, which is chemically identical to lovastatin. So yes - it works like a statin. And yes - it carries the same muscle risks. It’s not regulated like prescription drugs, so dosing is inconsistent. Some batches have dangerous levels of a toxin called citrinin. Don’t assume natural means safer. If you’re using it, tell your doctor. It can interact with the same drugs as prescription statins.
Can I restart a statin after stopping because of muscle pain?
Yes - but not the same one. Many people assume they’re “allergic” to statins. In reality, they just reacted to one type. Studies show 71% of people who stopped statins due to muscle pain can tolerate a different statin, especially at a lower dose. Try pravastatin or rosuvastatin. Start low. Go slow. Monitor symptoms. Most get back on track without issues.
Should I get genetic testing for SLCO1B1 before starting a statin?
The FDA added SLCO1B1 gene info to simvastatin labels in 2011 because people with a certain variant have a 4.5x higher risk of myopathy. But routine testing isn’t standard practice. It’s expensive, not widely available, and doesn’t change recommendations for most people. If you’ve had severe muscle pain on a statin before, ask your doctor about it. Otherwise, the safer approach is to start with a low-risk statin like pravastatin.



Comments (8)
Andrew Forthmuller
12 Nov 2025
statins are a nightmare for my quads. switched to pravastatin after my last doc gave me simva at 80mg and i couldnt walk up stairs. 2 weeks later, back to normal. dont be a hero, go low and slow.
vanessa k
13 Nov 2025
I know someone who went from feeling fine to needing a cane in 3 weeks because they didn't tell their pharmacist about the clarithromycin. It's not just about the statin-it's the combo. Please, if you're on anything else, say something. Your muscles will thank you.
manish kumar
14 Nov 2025
Let me tell you something-this whole statin-myopathy thing isn’t just about chemistry or genetics, it’s about how our bodies are wired to respond to foreign molecules. The liver isn’t just a filter-it’s a diplomat, negotiating between what’s needed and what’s toxic. When you throw in macrolides or fibrates, you’re essentially sending conflicting orders to that diplomat. The result? Muscle cells panic, start leaking, and suddenly you’re in the ER with CK levels through the roof. But here’s the beautiful part: the body remembers. If you switch to a hydrophilic statin, the diplomat gets a new script, and suddenly everything works again. It’s not that you’re intolerant-it’s that you were given the wrong language. Pravastatin isn’t a compromise; it’s a reset button.
Nicole M
15 Nov 2025
so grapefruit juice is bad for simva but fine for rosuvastatin? why does no one just say that upfront? i’ve been avoiding grapefruit for years thinking it was all statins. dumb.
Arpita Shukla
15 Nov 2025
Actually, the SLCO1B1 gene variant is only relevant in about 15% of the population, and most doctors don't even know how to interpret the results. Red yeast rice is a scam-it's literally unregulated lovastatin with added mold toxins. And no, CoQ10 doesn't help. The only thing that helps is knowing which statin you're on and which drugs you're mixing it with. Stop listening to internet advice and talk to a pharmacist.
Mark Rutkowski
17 Nov 2025
There’s something deeply human about this whole thing. We want a pill for everything-fast, easy, no consequences. But our bodies aren’t machines. They’re ecosystems. And when we mess with one part-like cholesterol production-we don’t just change a number, we ripple through every cell. The fact that 71% of people who think they’re ‘statin intolerant’ can actually tolerate another one? That’s not a failure of the drug. That’s a failure of the system. We hand out simvastatin like candy and then act shocked when someone’s legs give out. We need to start treating patients like people-not data points.
Ryan Everhart
18 Nov 2025
so you’re telling me the guy who takes 80mg simva + diltiazem + eats grapefruit… is basically playing Russian roulette with his kidneys? and we still let this happen? wow. just wow.
David Barry
19 Nov 2025
71% success rate on switching? That’s not a miracle-it’s a indictment of lazy prescribing. If your first-line statin is simvastatin and your patient is over 65, you’re not a doctor-you’re a liability. Pravastatin costs $6.60. It’s not hard. Stop being cheap and start being smart.