Eustachian Tube Dysfunction: Ear Pressure and Relief Options

Ever feel like your ears are stuffed with cotton, especially after a cold or during a flight? You’re not alone. Millions of people experience this strange, frustrating sensation - not from wax, not from infection, but from something hidden deep inside your head: the Eustachian tube is a narrow passageway that connects the middle ear to the back of the nose and throat, helping to balance pressure on both sides of the eardrum. Also known as the auditory tube, it opens briefly when you swallow, yawn, or chew. When it doesn’t, pressure builds up, and that’s when trouble starts.
What Exactly Is Eustachian Tube Dysfunction?
Eustachian Tube Dysfunction (ETD) happens when this tiny tube gets blocked or doesn’t open properly. Think of it like a valve that’s stuck shut. Normally, the middle ear is a sealed space. Air inside it slowly gets absorbed by the lining. Without fresh air coming in through the Eustachian tube, negative pressure builds up. That pulls the eardrum inward. The result? Fullness, muffled hearing, and sometimes even pain.
It’s not just about feeling weird. The pressure difference can reduce hearing by 15 to 40 decibels - enough to make conversations fuzzy. If it lasts more than three weeks, fluid can start pooling behind the eardrum. This is called serous otitis media. It’s not an infection, but it can make hearing even worse - up to 50 decibels lost. That’s like listening to someone talk from another room.
The good news? Most cases clear up on their own. About 70% of people feel better within two weeks without any treatment. But if it drags on, or if you’re in constant discomfort, you need to know what to do next.
What Does ETD Actually Feel Like?
People describe ETD in similar ways. It’s not the sharp, throbbing pain of an ear infection. It’s more like:
- A plugged-up feeling, like you’re underwater
- Hearing that sounds muffled, as if someone turned down the volume
- Clicking or popping noises when you swallow
- Ringing in the ear (tinnitus), especially when the pressure changes
- A slight dizziness or unsteadiness
Studies show 87% of patients report ear fullness. Nearly 92% have muffled hearing. And 78% notice popping or clicking. These aren’t rare side effects - they’re the norm. If you’ve had a cold and now your ear feels weird after you swallow, that’s likely ETD.
One big clue? Symptoms get worse during altitude changes. Flying, driving through mountains, or even riding in an elevator can make it feel like your ears are being crushed. That’s because the air pressure outside shifts, but the pressure inside your ear stays stuck. That 95% statistic isn’t an exaggeration - it’s what most people with ETD experience.
Why Does This Happen? The Real Causes
ETD isn’t random. It’s usually tied to something else. Here’s what triggers it most often:
- Upper respiratory infections - colds, flu, sinus infections. These cause swelling and mucus buildup. They’re behind 68% of cases.
- Allergies - pollen, dust, mold. They inflame the lining of the nose and throat, blocking the tube. This causes 22% of cases.
- Sinus infections - when the sinuses get infected, the inflammation spreads. This accounts for 10% of cases.
Children are especially prone. Their Eustachian tubes are shorter, more horizontal, and narrower. That makes them easier to block. Adults between 30 and 50 are also common sufferers - often because of chronic allergies or sinus issues.
There’s one rare but serious cause: a growth or tumor behind the eardrum or in the nasopharynx (the space behind the nose). This happens in less than 0.5% of cases. But if you have persistent ETD symptoms without any recent cold or allergy flare-up - especially if one ear is affected and the other isn’t - you should get it checked out.

How Is It Different From Other Ear Problems?
It’s easy to confuse ETD with other ear issues. Here’s how to tell them apart:
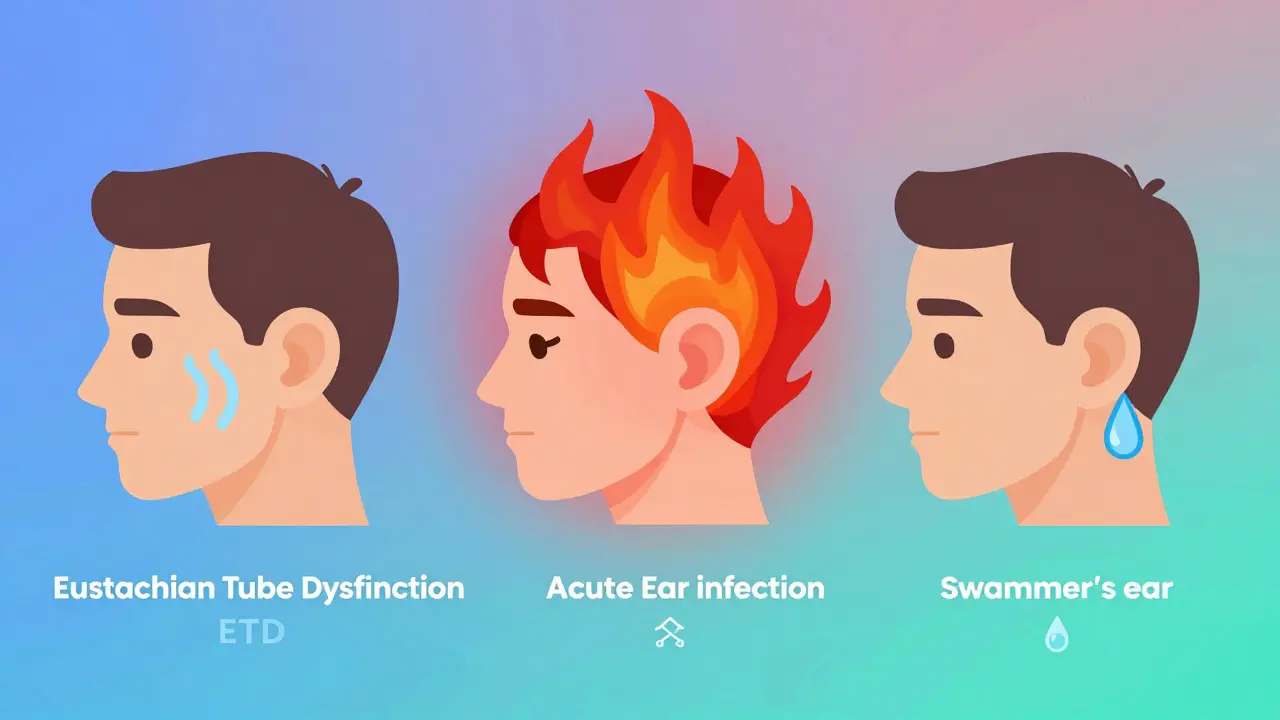
| Condition | Primary Symptom | Duration | Key Differentiator |
|---|---|---|---|
| Eustachian Tube Dysfunction (ETD) | Pressure, muffled hearing, popping | Days to weeks (can become chronic) | Worsens with altitude changes |
| Acute Otitis Media (Ear Infection) | Constant, severe ear pain | Usually resolves in 1-2 weeks | Pain doesn’t change with swallowing or yawning |
| Otitis Externa (Swimmer’s Ear) | Pain when touching outer ear | Days to weeks | Pain is outside the ear canal |
| Barotrauma | Sudden ear pain during pressure change | Hours to days | Only happens during flying or diving |
ETD doesn’t usually cause constant pain. If your ear hurts all the time, even when you’re not swallowing, it’s probably something else. And unlike barotrauma - which happens during a single event like a flight - ETD can stick around for weeks or months.
What Can You Do at Home? Simple Relief Methods
Before you reach for medicine, try these natural, proven methods. Most people find relief this way - especially in the first few days.
- Swallowing - Do it often. Every 15 to 20 minutes. Water helps. It triggers the muscles that open the tube.
- Chewing gum - Especially sugar-free. Chewing activates the muscles that pull the tube open. Do it for 10-15 minutes every 2 hours.
- Yawning - Force it if you have to. Opening your mouth wide stretches the muscles around the tube. 78% of people report relief from this.
- The Valsalva maneuver - Breathe in deeply, pinch your nose shut, and gently blow through your nose like you’re trying to pop your ears. Don’t blow hard. Just enough to feel pressure. Do this 3-5 times an hour. About 65% of users say it works - but 45% get it wrong the first time. Too much force can hurt your eardrum.
- Stay hydrated - Thinner mucus = easier flow. Drink water all day. Avoid caffeine and alcohol - they dry you out.
People who fly often swear by these. One Reddit user, u/FrequentFlyerMD, said: “The Valsalva maneuver works like magic for me during flights.” It’s not magic - it’s physics. You’re forcing air through the tube.
When to See a Doctor - And What They Do
If symptoms last longer than two weeks, or if you’re in real discomfort, it’s time to see an ear specialist. Most cases resolve on their own, but if they don’t, there are safe, effective options.
Doctors usually start with nasal sprays:
- Decongestant sprays (like oxymetazoline/Afrin) - These shrink swollen tissue. But don’t use them for more than 3 days. After that, they can make congestion worse.
- Steroid nasal sprays (like fluticasone/Flonase) - These reduce inflammation. Safe for longer use - typically 2 to 4 weeks. They’re the go-to for allergy-related ETD.
If these don’t help, you might be offered a procedure:
- Myringotomy - A tiny cut in the eardrum to drain fluid. Usually for kids or people with repeated fluid buildup. Temporary fix.
- Balloon dilation (BDET) - A tiny balloon is inserted into the Eustachian tube through the nose, inflated for 2 minutes, then removed. It stretches the tube open. Takes about 20 minutes, done in-office under local numbing. Studies show 67% success at 12 months. It’s becoming more common - usage jumped 220% between 2018 and 2022.
There’s no need for major surgery anymore. These minimally invasive options are changing how ETD is treated. The American Academy of Otolaryngology now advises against antibiotics for ETD unless there’s a clear infection. Most cases are about inflammation, not bacteria.
What Doesn’t Work - And Why
There’s a lot of misinformation out there. Here’s what to avoid:
- Ear candles - They don’t work. They’re dangerous. Don’t risk burns or eardrum damage.
- Over-the-counter ear drops - Unless prescribed, they won’t help. ETD is not an ear canal issue.
- Blowing your nose too hard - This can force mucus into the middle ear and make things worse.
- Ignoring persistent pain - If your ear hurts constantly, it’s not ETD. It could be an infection or something else. See a doctor.
One common mistake? People think decongestants will fix everything. But if your ETD is from allergies, decongestants won’t touch the root cause. Steroid sprays do. That’s why identifying the trigger matters.
Long-Term Outlook - Can ETD Become Chronic?
Yes. If symptoms last more than three months, it’s considered chronic. That’s harder to treat. But it’s not hopeless.
Chronic ETD often means the tube has become scarred or narrowed over time. That’s where balloon dilation shines. It physically widens the tube. Early results show 72% effectiveness at six months. New research is looking at bioabsorbable stents - tiny, dissolvable supports that keep the tube open. Early trials show 85% symptom improvement in three months.
And the trend is clear: more people are getting relief without surgery. Minimally invasive procedures are growing by 15% per year. By 2026, they’ll be the standard for persistent ETD.
The good news? ETD is rarely permanent. Even chronic cases respond well to treatment. The key is not waiting too long. If you’ve tried the basics for two weeks and it’s still there - don’t suffer. See a specialist. There’s help.
Can Eustachian tube dysfunction cause permanent hearing loss?
No, not usually. If ETD is treated before fluid builds up for months, hearing typically returns to normal. Long-term blockage (over 3 months) can lead to fluid buildup and temporary hearing loss of up to 50 decibels. But once the pressure is equalized and fluid drains - whether naturally or with treatment - hearing usually comes back. Permanent damage is rare and only happens if the eardrum or inner ear structures are damaged by prolonged, untreated pressure.
Why does my ear pop when I swallow?
That popping is the Eustachian tube opening. When you swallow, the muscles around the tube contract and pull it open, letting air flow in or out to balance pressure. In ETD, this doesn’t happen smoothly - so the tube snaps open suddenly, creating a popping sound. It’s your body’s way of trying to fix the pressure imbalance. If it happens often, it’s a sign the tube is struggling to function normally.
Can allergies cause Eustachian tube dysfunction?
Yes - and it’s one of the top causes. Allergies make the lining of the nose and throat swell. This swelling can block the opening of the Eustachian tube. If you notice your ears feel blocked during allergy season, or after being around pollen or dust, your ETD is likely allergy-related. Steroid nasal sprays are often the most effective treatment in these cases.
Is it safe to use the Valsalva maneuver every day?
It’s safe to use occasionally - like during flights or when you feel pressure building. But doing it aggressively or multiple times an hour for weeks can strain your eardrum or force mucus into the middle ear. Use gentle pressure. If you’re not getting relief after a few days, stop and try other methods. Overuse doesn’t help - it can hurt.
Why do children get ETD more often than adults?
Children’s Eustachian tubes are shorter, more horizontal, and narrower than adults’. This makes them easier to block with mucus or swelling. Their immune systems are also still developing, so they get more colds and infections - the main trigger for ETD. That’s why ear issues are so common in kids under 7. As they grow, the tubes become more angled and wider, reducing the risk.



Comments (10)
Matt Alexander
4 Mar 2026
Just wanted to say the chewing gum trick works wonders. I fly twice a month and used to dread the pressure. Now I chew sugar-free gum the whole flight. No more muffled hearing. Simple, free, and it actually works. No magic, just physics.
Dean Jones
5 Mar 2026
What fascinates me about ETD isn't just the mechanics, but how our bodies are designed to self-correct. The fact that swallowing, yawning, even just sipping water can trigger a neural-muscular reflex that equalizes pressure across a sealed cavity is breathtaking. It's evolutionary engineering at its finest. And yet we treat it like a nuisance instead of marveling at the fact that our ears are constantly balancing atmospheric pressure without us even thinking about it. Most people don't realize their body is a living barometer. The Eustachian tube is nature's pressure valve, and when it fails, it's not a disease-it's a system overload. We're talking about a structure so delicate it can be blocked by a single puff of pollen, yet so vital that its failure can mute the world. We take it for granted until we can't hear our own thoughts.
Gretchen Rivas
7 Mar 2026
Steroid sprays saved me. Allergy season hit hard last year, ears felt like they were wrapped in plastic. Flonase for three weeks-no more popping, no more muffled speech. Don’t skip the doctor if it lingers.
Mike Dubes
8 Mar 2026
Yall need to stop with the valseva like its a sport. I did it 10 times an hour for a week trying to 'fix' my ear and ended up with a ruptured eardrum. No joke. Doc said i was being a dumbass. Gentle pressure only. And drink water. Always. Caffeine is the enemy.
John Cyrus
8 Mar 2026
Anyone who recommends ear candles is either a scammer or an idiot. There's zero science behind it. Just because some influencer posted a video of wax coming out doesn't mean it worked. That wax was from the candle not your ear. And don't even get me started on OTC drops. ETD isn't an ear canal problem. It's a pressure valve issue. Stop wasting money on snake oil.
John Smith
8 Mar 2026
ETD is the silent thief of clarity. You don't realize how much you rely on crisp sound until it's gone. One day you're laughing at a joke, next day you're nodding like a robot because you heard 'uhhh' instead of 'that's hilarious.' It's not just hearing loss-it's emotional isolation. I didn't cry until I missed my kid saying 'I love you' because my ear was stuck. Don't wait. Fight it. Steroid spray. Hydration. Chewing. Don't let your ears become a prison.
Shivam Pawa
10 Mar 2026
From India, where seasonal allergies are brutal. I've had chronic ETD for 5 years. Balloon dilation changed everything. Procedure took 18 minutes. Local numbing. No downtime. Now I can fly without anxiety. The stats are real. 67% success at 12 months. I'm in that group. Also, avoid dairy during congestion. Thickens mucus. Simple but overlooked.
Lebogang kekana
11 Mar 2026
Bro, I thought I was going deaf during that flight to Cape Town. Felt like my head was in a vice. Tried everything. Then I remembered the yawn trick. Forced a yawn. POP. Like a switch flipped. Tears in my eyes. Not from pain-from relief. ETD is a monster but it's beatable. Stay strong. Your ears are fighting for you. Don't give up.
Jessica Chaloux
11 Mar 2026
Thank you for writing this. I’ve been so scared. I thought it was something serious. I cried last night because I couldn’t hear my dog bark. I’m trying the gum and water now. I feel hopeful for the first time in weeks 🥹💧
Raman Kapri
13 Mar 2026
While the provided information contains numerous empirical claims, one must question the statistical generalizations presented. For instance, the assertion that '70% of people feel better within two weeks' lacks citation from peer-reviewed longitudinal studies. Furthermore, the efficacy of balloon dilation at 67% is derived from industry-funded trials with small sample sizes. Until independent replication occurs, such claims remain speculative. Medical intervention should not be predicated on anecdotal Reddit testimonials or marketing-driven statistics.