Glaucoma Medications: Prostaglandins vs. Beta Blockers & Safety Guide
Imagine waking up one day to find your peripheral vision slowly fading away, like a curtain being drawn across your world. This is the silent threat of glaucoma, a condition that damages the optic nerve and often goes unnoticed until significant vision loss has occurred. For millions of people worldwide, the primary defense against this damage isn't surgery or lifestyle changes-it's a daily routine involving eye drops. But not all drops are created equal. You might be prescribed prostaglandin analogs (PGAs) or beta-blockers, two powerful classes of medication that work in completely different ways to lower intraocular pressure (IOP).
Choosing between them isn't just about which one lowers pressure better; it's about how each drug affects your body, your eyes, and your daily life. One class works once a day with cosmetic side effects, while the other requires twice-daily dosing and carries risks for your heart and lungs. Understanding these differences is crucial for anyone managing glaucoma, as adherence to the treatment plan is the single biggest factor in preventing blindness.
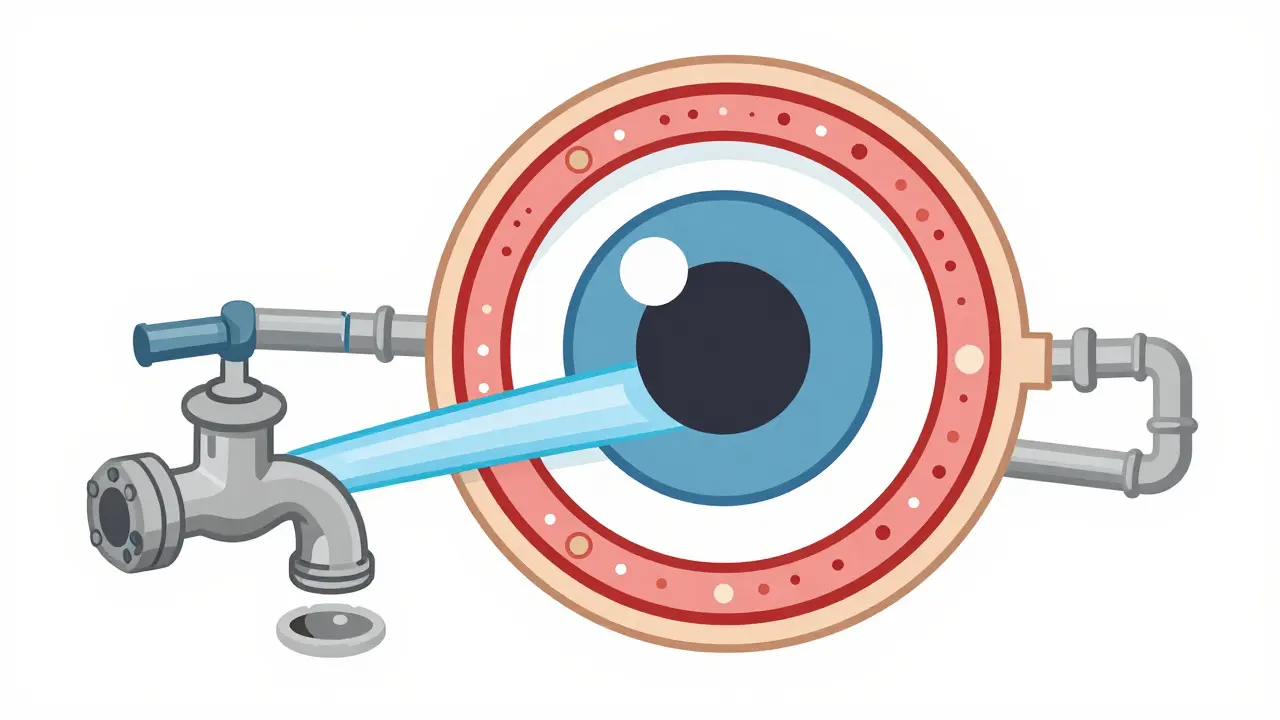
How Glaucoma Medications Work: The Plumbing Analogy
To understand why you need specific drops, think of your eye like a sink. Water (aqueous humor) constantly flows into the eye, and there must be a drain to let it out. In healthy eyes, the inflow and outflow are balanced, keeping the water level (pressure) stable. In glaucoma, either too much water enters, or the drain gets clogged, causing pressure to build up. This high pressure squeezes the delicate optic nerve at the back of the eye, leading to irreversible damage.
Prostaglandin analogs, such as latanoprost, bimatoprost, and travoprost, act on the "drain." Specifically, they increase uveoscleral outflow-the pathway through which fluid exits the eye tissue. They do this by relaxing the muscles around the drainage channels, allowing more fluid to escape. Because they target the exit route, they are highly effective at lowering pressure without stopping the production of new fluid.
In contrast, Beta-blockers, like timolol and betaxolol, act on the "faucet." They inhibit the ciliary body from producing aqueous humor. By reducing the amount of fluid entering the eye, the overall volume decreases, and so does the pressure. While both methods effectively lower IOP, their mechanisms dictate very different safety profiles and side effect patterns.
| Feature | Prostaglandin Analogs (PGAs) | Beta-Blockers |
|---|---|---|
| Dosing Frequency | Once daily | Twice daily |
| Mechanism | Increases fluid outflow | Decreases fluid production |
| IOP Reduction | 24-33% | 20-25% |
| Key Side Effects | Iris darkening, eyelash growth, redness | Fatigue, respiratory issues, slow heart rate |
| Adherence Rate | Higher (easier routine) | Lower (complex routine) |
Prostaglandin Analogs: The First-Line Choice
If you visit an ophthalmologist today for newly diagnosed primary open-angle glaucoma, there is a strong chance they will prescribe a prostaglandin analog first. Why? Because they are simply more convenient and generally safer for most patients. Latanoprost, introduced in 1996, revolutionized glaucoma care by proving that a single drop per night could control pressure effectively.
The efficacy is impressive. Studies show PGAs can reduce intraocular pressure by 24% to 33% from baseline levels. This makes them superior to many older treatments. However, convenience comes with a visual cost. These drugs are prodrugs that become active after penetrating the cornea, and they stimulate melanocytes (pigment cells) in the iris. Over time, this can cause your eye color to darken permanently. If you have light-colored eyes-blue, green, or hazel-you might notice a shift toward brown. This change is usually gradual but irreversible.
Another unexpected side effect is hypertrichosis, or excessive hair growth. Many users report thicker, longer, and darker eyelashes. While some view this as a bonus beauty benefit, others find the accompanying ocular irritation uncomfortable. Redness (hyperemia) occurs in 30% to 50% of users, and a burning sensation is common, particularly with bimatoprost, which is known to be more irritating than latanoprost.
Beta-Blockers: Potent but Systemic Risks
Beta-blockers have been a staple in glaucoma treatment for decades. Timolol maleate 0.5% is perhaps the most recognized name in this class. It works by blocking beta-adrenergic receptors in the ciliary body, slowing down the production of aqueous humor. It typically lowers IOP by 20% to 25%, which is effective but slightly less potent than top-tier PGAs.
The major drawback of beta-blockers is systemic absorption. Even though you put the drop in your eye, the fluid drains through the nasolacrimal duct into your nose and throat, where it enters your bloodstream. This means the drug affects your entire body, not just your eye. For patients with asthma, chronic obstructive pulmonary disease (COPD), or certain heart conditions, this can be dangerous. Beta-blockers can trigger bronchospasm (tightening of the airways) or slow the heart rate excessively.
Because of these risks, doctors must screen patients carefully before prescribing timolol. Fatigue is another common complaint, reported by 15% to 20% of users. Additionally, because beta-blockers require twice-daily administration, adherence rates drop significantly compared to once-daily PGAs. Missing doses leads to fluctuating pressure, which can still damage the optic nerve even if the average pressure seems okay.
Safety Profiles and Preservative Concerns
When discussing safety, we cannot ignore preservatives. Most multi-dose eye drop bottles contain benzalkonium chloride (BAK) to prevent bacterial growth. Long-term use of BAK can damage the surface of the eye, leading to dry eye syndrome, inflammation, and discomfort. A 2021 meta-analysis in Acta Ophthalmologica found that preservative-free formulations significantly improved tear break-up time and Schirmer's test results, indicating better ocular surface health.
However, the trade-off is price and stability. Preservative-free options are often single-use vials or specialized bottles that are 20% to 25% more expensive. Interestingly, the study noted that the difference in actual IOP reduction between preserved and preservative-free versions was minimal (less than 0.3 mmHg). So, while preservative-free drops are gentler on the eye surface, they don't necessarily lower pressure better. For long-term users with sensitive eyes, the extra cost may be worth the comfort, but for others, standard preserved drops remain a viable option.
Another safety concern for prostaglandins is cystoid macular edema (CME), a swelling in the center of the retina. This is rare in healthy eyes but poses a risk for pseudophakic patients (those who have had cataract surgery) or those with a history of uveitis. The incidence rate is low (0.5% to 1.0%), but it’s a critical consideration for post-surgical patients.
Combination Therapies and Adherence
What happens when one drop isn't enough? Many patients eventually require combination therapy. Research shows that combining a PGA with a beta-blocker (like latanoprost and timolol) has a synergistic effect, lowering IOP by an additional 13% to 25% beyond what either drug achieves alone. This additivity is clinically significant.
However, adding a second bottle doubles the complexity of your routine. Adherence rates drop by 15% to 20% when patients must manage multiple medications. To combat this, fixed-combination drops exist, mixing two drugs into one bottle. While convenient, clinical trials have not consistently shown that fixed combinations are more effective than using two separate drops correctly. The real benefit is psychological: fewer bottles mean fewer chances to forget a dose.
Crucially, you should never combine two different prostaglandins (e.g., bimatoprost and latanoprost). Unlike mixing a PGA with a beta-blocker, using two PGAs together can paradoxically increase intraocular pressure in some patients, making the condition worse. This practice is controversial and generally not recommended.
Making the Right Choice for Your Eyes
So, which medication is right for you? There is no universal answer, but here are some heuristics to discuss with your doctor:
- Choose PGAs if: You want a simple once-daily routine, have no contraindications to pigment changes, and prioritize high efficacy with minimal systemic risk.
- Consider Beta-Blockers if: Cost is a major factor (they are often cheaper generics), you have severe ocular surface disease that reacts poorly to PGAs, or you need rapid initial pressure control alongside other therapies.
- Avoid Beta-Blockers if: You have asthma, COPD, bradycardia (slow heart rate), or heart block. Always disclose your full medical history.
- Monitor Closely if: You have had cataract surgery or have a history of eye inflammation, due to the CME risk with PGAs.
Ultimately, the best medication is the one you actually use. Since PGAs have higher persistence rates (patients stick with them longer), they are often the preferred starting point. But if side effects like redness or irritation make you stop taking them, the pressure will rise, and the vision loss will continue. Regular follow-ups are essential to monitor both pressure levels and any emerging side effects.
Can glaucoma eye drops cure glaucoma?
No, glaucoma eye drops cannot cure the disease. They manage the symptoms by lowering intraocular pressure, which slows or halts further damage to the optic nerve. Any vision already lost is permanent. Consistent use is required indefinitely to preserve remaining sight.
Why do my eyes turn brown with prostaglandin drops?
Prostaglandin analogs stimulate melanocytes in the iris to produce more pigment. This is a permanent change, especially noticeable in people with lighter eye colors like blue or green. It does not affect vision quality but is a cosmetic side effect that continues as long as you use the medication.
Are beta-blocker eye drops safe for asthmatics?
Generally, no. Non-selective beta-blockers like timolol can absorb systemically and constrict airways, triggering bronchospasm in patients with asthma or COPD. Doctors usually avoid these for respiratory patients or use cardioselective alternatives with extreme caution.
Should I switch to preservative-free eye drops?
If you experience chronic dry eye, stinging, or redness unrelated to the drug's mechanism, preservative-free options may help. They are gentler on the ocular surface. However, they are more expensive and require different storage. Discuss this with your ophthalmologist to see if the comfort improvement justifies the cost.
Can I use two different prostaglandin drops together?
No, combining two prostaglandin analogs (such as latanoprost and bimatoprost) is not recommended. Studies suggest this combination can potentially increase intraocular pressure rather than lower it, worsening your glaucoma. Always follow your doctor's specific combination instructions.




Comments (10)
Sumit gupta
24 Jun 2026
pretty chill breakdown of the meds. i always forget which one does what until someone explains it like this.
Jake Kitzmiller
26 Jun 2026
The plumbing analogy is actually spot on for explaining IOP dynamics to patients who aren't medical professionals. It simplifies the complex physiology of aqueous humor production and outflow without losing accuracy. Many people struggle with adherence because they don't understand why twice-daily dosing is necessary for beta-blockers versus once-daily for PGAs. The systemic absorption issue with timolol is also a critical point that gets overlooked in casual discussions. Patients with mild asthma often don't realize how dangerous non-selective beta-blockers can be until they experience bronchospasm. It's great to see this information laid out clearly for public consumption.
Annemarie Kautz
26 Jun 2026
ugh another article about eye drops... i hate them so much :(
Dale Simpson
28 Jun 2026
hey everyone! just wanted to say that staying on top of these drops is super important even if they feel annoying sometimes. u got this! keep fighting the good fight for your vision!
alexander barrera
28 Jun 2026
Only Americans would need such a long explanation for basic medicine 🇺🇸💊 We should just trust our doctors blindly instead of reading internet blogs. This is peak western dependency culture right here. Stop whining about side effects and take your pills like adults do in civilized nations. 😒
Charlotte Stuart
29 Jun 2026
This article is fundamentally flawed in its presentation of clinical data. The comparison table oversimplifies the nuanced pharmacokinetics involved in prostaglandin analogs versus beta-adrenergic antagonists. Furthermore, the suggestion that preservative-free options are merely a matter of 'comfort' ignores the significant clinical implications of benzalkonium chloride-induced toxicity in chronic glaucoma patients. One must consult peer-reviewed journals rather than rely on such superficial summaries.
Hema Khimasia
29 Jun 2026
The dichotomy between symptomatic management and curative intervention highlights the epistemological limits of current ophthalmological therapeutics. While prostaglandin analogs modulate uveoscleral outflow effectively, they merely mitigate the progression of optic neuropathy rather than reversing established axonal loss. This necessitates a philosophical reconsideration of 'success' in chronic disease management, where stability is prioritized over restoration. The systemic bioavailability of topical beta-blockers further complicates the risk-benefit analysis, introducing variables that extend beyond ocular hemodynamics into general cardiovascular physiology.
krystal Live
1 Jul 2026
you guys are doing great by reading up on this stuff! knowledge is power when it comes to health. dont let the side effects scare you off from protecting your sight. we believe in you!!
Tucker Brown
3 Jul 2026
I suspect the pharmaceutical companies are pushing prostaglandins not because they are better but because the patent structures allow for higher margins compared to generic beta-blockers. The 'cosmetic' side effects are likely underreported to maintain sales volume. Always question the source of funding behind these 'guides'. They want you dependent on their specific brand of drops.
Alyssa Smith
4 Jul 2026
It is really helpful to have all this information in one place. Understanding the differences helps make better decisions with your doctor. Stay positive and keep up with those appointments!